Arthroscopy (ar-THROS-ka-pea) is an outpatient surgical procedure used by orthopaedic surgeons to diagnose and treat problems inside a joint. The surgeon makes small incisions, less than half an inch long, and inserts a pencil-sized instrument called an arthroscope. The arthroscope contains a small lens, a miniature camera and a lighting system.
This projects three-dimensional images of the joint on a television monitor, enabling the surgeon to look directly inside the joint and identify the trouble. Tiny probes, forceps, knives and shavers can then be used to correct many problems at the same time.
Arthroscopy has been used for several years to treat conditions in large joints such as the knee and the shoulder. As cameras and instruments became smaller and more refined, arthroscopy was applied to other joints, including the wrist. The wrist is a complex joint, with eight small bones and many connecting ligaments. Arthroscopy enables the surgeon to see the anatomic parts and their movements and to make a more accurate diagnosis.
Diagnostic arthroscopy
Diagnostic arthroscopy may be used if the cause of your wrist pain cannot be identified or if wrist pain continues for several months despite nonsurgical treatment.
Before surgery, your doctor will do:
- A physical examination that focuses on your hand and wrist. Your doctor will also ask about your medical history.
- Provocative tests that involve moving your hand in ways that reproduce the pain.
- Imaging studies, such as X-rays of your hand and wrist. In some cases, additional imaging studies may be needed. These can include an MRI (magnetic resonance image) or an arthrogram, in which a contrast agent is injected into the joint before the image is taken.
Usually, regional anesthesia is used during arthroscopic surgery. This numbs your arm and hand. You may also be given a sedative to further relax you and enable you to doze through the surgery. Two or more small incisions (portals) are made on the back of the wrist, through which the arthroscope and instruments are inserted. After the surgery, the incisions are closed with a small stitch and a dressing is applied. Sometimes a splint may also be used.
Arthroscopic surgical treatment
Several conditions can be treated using arthroscopic surgery, including chronic wrist pain, wrist fractures, ganglion cysts and tears in the ligaments or the triangular fibrocartilage complex (TFCC). Wrist arthroscopy may also be used to smooth the bone surfaces and remove inflamed tissue. Arthroscopy can also be used to surgically treat carpal tunnel syndrome, but in that diagnosis, the arthroscope is not inserted into the wrist joint itself.
- Chronic wrist pain: Arthroscopic exploratory surgery may be used to diagnose the cause of chronic wrist pain when other tests are inconclusive. Often, there may be areas of inflammation, cartilage damage, or other findings after a wrist injury. In some cases, after the diagnosis is made, the condition can be treated arthroscopically as well.
- Wrist fractures: Doctors can remove small fragments and fracture debris, align the broken pieces of bone, and stabilize them by using pins, wires, or screws.
- Ganglion cysts: These cysts commonly grow from a stalk between two of the wrist bones. During an arthroscopic procedure, the surgeon can remove the stalk, which may also reduce recurrence of the cysts.
- Ligament/TFCC tears: Ligaments are fibrous bands of connective tissue that link or hinge bones. They provide stability and support to the joints. The TFCC is a cushioning structure within the wrist. A fall on an outstretched hand can tear ligaments, the TFCC or both, resulting in pain with movement or a clicking sensation. During arthroscopic surgery, the surgeon can trim or repair the tears.
- Carpal tunnel release: Carpal tunnel syndrome is characterized by numbness or tingling in the hand, and sometimes with pain up the arm. It is caused by pressure on a nerve that passes through the carpal tunnel, which is formed by the wrist bones and a thick tissue roof. Pressure can build up within the tunnel for many reasons, including irritation and swelling of the tissue (synovium) that covers the tendons. If the syndrome does not respond to conservative treatment, your doctor may recommend surgery to cut the ligament roof and enlarge the tunnel, thus reducing pressure on the nerve and relieving symptoms. This can sometimes be done using an arthroscope.
After surgery, you will need to keep your wrist elevated for the first two or three days and keep your bandage clean and dry. You can ice your wrist to help keep swelling down. Your doctor and/or your physical therapist will teach you exercises to help maintain motion and rebuild your strength. Analgesic medications will help relieve any postoperative pain, which is usually mild.
Complications
Complications during or after arthroscopic wrist surgery are unusual, but may include infection, nerve injuries, excessive swelling or bleeding, scarring or tendon tearing. An experienced surgeon, particularly one who specializes in treating the hand, can reduce the likelihood of complications.
Summary
Arthroscopic surgery is a valuable diagnostic and treatment tool. It is minimally invasive, and patients generally experience fewer problems and a more rapid recovery than with open surgery. Because it is an outpatient procedure, most patients are home several hours after surgery.
 Description
Description 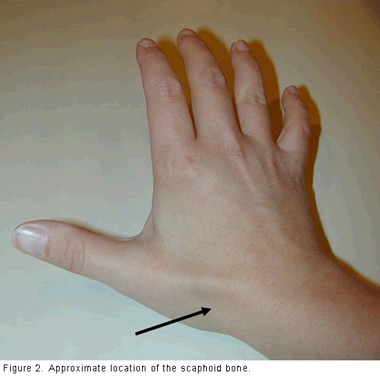 Sometimes, a broken scaphoid does not show up on an X-ray right away. When this is the case, the doctor may put your wrist in a splint and wait to take a new X-ray in a week or two, when the fracture may become visible. Keep the splint on and do not do any heavy lifting during the waiting time.
Sometimes, a broken scaphoid does not show up on an X-ray right away. When this is the case, the doctor may put your wrist in a splint and wait to take a new X-ray in a week or two, when the fracture may become visible. Keep the splint on and do not do any heavy lifting during the waiting time.