
 Anatomy
Anatomy
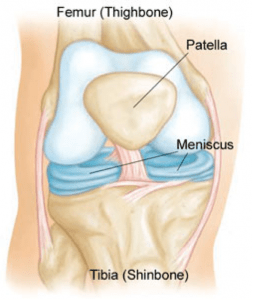
Between the femur and tibia, sitting centrally in the knee joint, are two C-shaped pads (the medial and lateral menisci) that act as a cushion or shock absorber between the two bones.
The meniscal pads are made of cartilage. The meniscus has a poor blood supply except on the very periphery of the meniscus.
Peripheral tears, although rare, can be repaired, especially in the younger patients. With the inner portion of the meniscus having a poor blood supply, the meniscus has little healing potential, which leads many tears to surgery to help resolve the symptoms.
Injury Mechanism
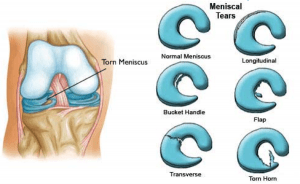 The meniscus is often injured with twisting the knee while in a squatting position. This creates a split or flap to occur while the meniscus is being compressed.
The meniscus is often injured with twisting the knee while in a squatting position. This creates a split or flap to occur while the meniscus is being compressed.
In younger patients, the meniscus is firm and is usually injured in sports activities. In older patient, the meniscus is often more brittle or friable and injuries can occur with daily activities such as squatting down to make the bed or working in the yard.
Symptoms
The “classic” meniscal injury creates pain on one side of the knee or in the back of the knee. The pain is usually worsened with more rigorous activities or with bending the knee fully. Bending the knee causes the meniscus to become pinched between the two bones. Meniscal tears can cause subtle mechanical symptoms like clicking.
However, sometimes patients will describe catching or actual “locking up” of the knee in which they cannot fully bend or straighten the knee. Swelling does not typically occur until several days after the injury and commonly with activities. Unlike with ACL injuries, the swelling will not usually subside until the meniscus tear is addressed surgically.
Diagnosis
The physician’s work-up will start with a careful history and exam. Sometimes patients recall a twisting injury when the pain began, but often patients just noticed that the knee began to hurt or swell with activities and cannot recall a specific event. On examination, the knee is often slightly swollen (effusion). Range of motion is often limited, and pain can usually be elicited with fully bending the knee. The knee is often tender on one side of the knee or the other specifically at the joint line.
X-rays are often obtained to see that no fractures have occurred with the injury and to help assess the overall condition of the knee joint. If significant arthritis is present, the outcome from surgery is less favorable even with a co-existing meniscus tear. An MRI scan is often obtained to confirm the diagnosis and to evaluate any associated injuries to the other meniscus, ligaments, or damage to the joint surfaces. Plain x-rays show the bones of the knee, while MRI scans reveal the soft tissues around the knee including the ligaments, menisci, muscles and tendons.
Treatment
Your physician will discuss treatment options with you. Treatment decisions are based on age, activity level, severity of symptoms, and associated arthritis within the knee. Often your surgeon will recommend surgery, since meniscus tears rarely heal without surgery, because of the poor blood supply mentioned above. In older patients with less activity demands and less severe symptoms, one can try nonoperative treatment including rest, ice, anti-inflammatories, occasional injections and see if the symptoms become tolerable.
In younger, more active patients, surgery is almost always recommended. Surgery involves removing or repairing the torn meniscal tissue. Most of the tears are in the central portion of the meniscus where there is no blood supply, therefore no healing potential. Those tears need to be removed, such as trimming off a hangnail. The surgeon tries to be conservative and only remove the damaged tissue so that adequate padding remains in the knee.
In the tears that are further out near the edge of the meniscus, where there is some healing potential, sutures can be placed through the arthroscope to repair the torn meniscus.
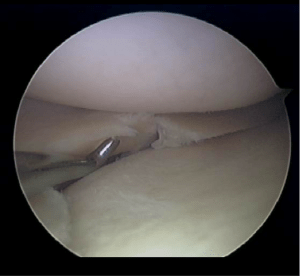
Probe shows tear in the meniscus
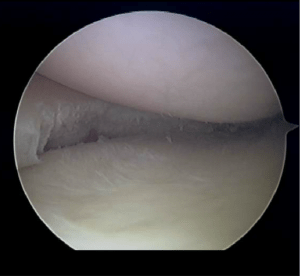
Same meniscus after removing the tear
What to expect after surgery
Meniscus surgery is performed as an outpatient procedure. The surgery takes about 30 minutes. Most patients are able to walk on their knee to the bathroom and meals even on the day of surgery without crutches, but most of the first day is spent resting with the leg elevated and iced. By the second or third day, most patients are able to drive and walk short distances and return to desk jobs.
By one week, patients are encouraged to start light, straight ahead exercising, such as using a stationary bike, an elliptical or stair climber, level walking or swimming. Activities are added during the next 2 to 3 weeks. By one month following surgery, most patients have returned to full activities. If the meniscus has been repaired rather than resected, a more prolonged recovery might become necessary to protect the repair.