Syndesmosis
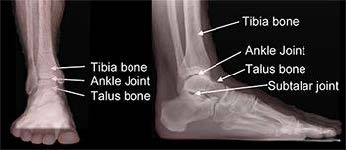
The two bones in the lower leg are the tibia and the fibula. The point just above the ankle where these two bones meet is called the syndesmosis. While technically a joint, it does not function like most joints as there is very little motion between the two bones. Its main functions are to provide stability to the ankle joint and to allow the joint to move.
The most common way the syndesmosis gets hurt is from a twisting or rotational injury to the ankle. The ligaments that support the syndesmosis are needed to stabilize it, and it is these ligaments that are stretched or torn when this type of injury occurs. Ankle sprains can injure the syndesmosis. The ligaments also can be injured when the ankle is broken. High ankle sprains that are commonly seen in football players are injuries to the syndesmosis.
Surgery of the syndesmosis most often is needed after a traumatic disruption. The goal of surgery is to properly align and stabilize the joint so the ligaments can heal in the correct position.
Diagnosis
Your foot and ankle orthopedic surgeon will examine your ankle. X-rays will be taken and may include a stress X-ray. This is an X-ray that is taken while your doctor carefully twists or stresses your ankle to test the stability of the syndesmosis. If there is an unstable joint, surgery is typically necessary to provide stability.
If the syndesmosis is found to be stable, it usually will not require surgical management. If you have other medical conditions that make surgery too risky for your health, your surgeon may recommend non-surgical treatment. Surgery should also be avoided if you have any active infections or chronic wounds around your ankle.
Treatment
Surgery usually is done on an outpatient basis, but sometimes an overnight stay is required. A general anesthetic typically is used and a nerve block may also be used during surgery or to provide pain relief after surgery. Your surgeon will put the syndesmosis into its proper position and secure it in place with screws or suture implants. A plate also may be used. Some foot and ankle orthopedic surgeons also look inside the ankle joint with an arthroscope to see if the cartilage is injured.
Specific Technique
After making an incision over the outside of the ankle, your surgeon will identify and expose the fibula bone and syndesmosis. Using direct vision and live X-ray techniques, your surgeon will place the syndesmosis into the correct position and set it with an implant. This typically involves one or two screws that go from the fibula bone into the tibia bone. The screws may be placed through a plate that sits on the fibula bone. Alternatively, your surgeon may use a suture device instead of screws.
A stress X-ray is performed to confirm that the syndesmosis is stable. Any additional injuries (e.g., fractures) are repaired if necessary. Your surgeon will close the incision(s) with stitches and then place your let in a splint, cast, or boot.
Recovery
After surgery, you may be immobilized in a splint for the first 10-14 days. You will typically be kept non-weightbearing for 6-8 weeks and then allowed to put weight on your foot in a cast or boot. Swelling persists for many months after this surgery. Stiffness can be problem and physical therapy often is necessary.
Risks and Complications
All surgeries come with possible complications, including the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots.
The main complications that can occur after this surgery include irritation or failure of the hardware, the development of arthritis in the syndesmosis, and failure of the syndesmosis to heal properly.
FAQs
Does my hardware need to be removed?
Most of the time, orthopedic hardware does not need to be removed. In the case of syndesmosis surgery, your surgeon may recommend removing the screws that go from the fibula to the tibia. Because there normally is motion between these two bones, the screws may cause pain or limit motion. The hardware is not removed until after the syndesmosis is healed. You and your surgeon will discuss what is best for you.