The posterior tibial tendon helps hold up your arch and provides support as you step off on your toes when walking. If this tendon becomes inflamed, overstretched, or torn, you may experience pain on the inner ankle and gradually lose the inner arch on the bottom of your foot, leading to a flatfoot deformity.
Symptoms
The symptoms of progressive flatfoot are gradual and typically include pain and swelling on the inside or outside of the ankle or foot, loss of the arch and the development of a flat foot, weakness and an inability to stand on the toes, and tenderness over the midfoot, especially during physical activity.
Causes
Progressive flatfoot often occurs in women over 50 and may be due to an inherent abnormality of the tendon. But there are several other risk factors, including:
- Obesity
- Diabetes
- Hypertension (high blood pressure)
- Previous surgery or trauma, such as an ankle fracture, on the inner side of the foot
- Local steroid injections
- Inflammatory diseases such as Reiter’s syndrome, rheumatoid arthritis, spondylosing arthropathy, and psoriasis
- Athletes who are involved in sports such as basketball, tennis, soccer, or hockey may tear the posterior tibial tendon. The tendon may also become inflamed if excessive force is placed on the foot, such as when running on a banked track or road.
Diagnosis
The diagnosis is based on both a history and a physical examination. Your foot and ankle orthopedic surgeon may ask you to stand on your bare feet facing away from him/her to view how your foot functions.
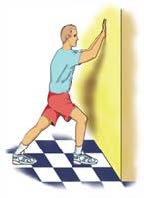
You also may be asked to stand on your toes or to do a single heel raise. You will stand with your hands on the wall, lift the unaffected foot off the ground, and raise up on the toes of the other foot. Normally, the heel will rotate inward; if not, this indicates posterior tibial tendon dysfunction. Your surgeon may request X-rays or an MRI of the foot.
Treatments
Without treatment, the flatfoot that develops from posterior tibial tendon dysfunction eventually becomes arthritic and rigid. Pain increases and spreads to the outer side of the ankle. The way you walk may be affected and wearing shoes may be difficult.
The treatment your surgeon recommends will depend on how far the condition has progressed. In the early stages, posterior tibial tendon dysfunction can be treated with rest, non-steroidal anti-inflammatory drugs such as aspirin or ibuprofen, and immobilization of the foot for 6-8 weeks with a boot to prevent overuse. After the boot is removed, shoe inserts such as a heel wedge or arch support may be helpful. If the condition is advanced, your doctor may recommend that you use a custom-made ankle-foot orthosis or support.
If conservative treatments don’t work, your doctor may recommend surgery. Several procedures can be used to treat progressive flatfoot; often more than one procedure is performed at the same time. Your doctor will recommend a specific course of treatment based on your foot. Surgical options include:
Osteotomy: This procedure changes the alignment of the calcaneus (heel bone). The surgeon may sometimes have to remove a portion of the bone.
Tendon transfer: This procedure uses some fibers from another tendon (the flexor digitorum longus, which helps bend the toes) to repair the damaged posterior tibial tendon.
Lateral column lengthening: In this procedure, the surgeon removes a small wedge-shaped piece of bone from either your hip or that of a cadaver and places it into the outside of the heel bone. This helps realign the bones and recreate the arch.
Arthrodesis: This procedure fuses one or more bones together, eliminating movement in the joint. This stabilizes the hindfoot and keeps the condition from progressing further.