 Anatomy
Anatomy
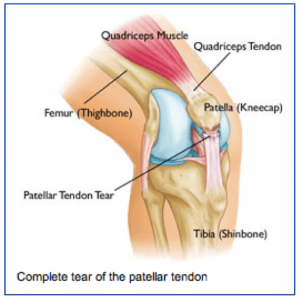
The quadriceps tendon attaches the main group of muscles in the front of the thigh (quadriceps) to the upper pole of the kneecap (patella).
The quadriceps muscle attaches to the upper pole of the kneecap through the quadriceps tendon to allow one to straighten out their leg or to support ones weight while squatting. When the quadriceps tendon is torn, one cannot support their weight when the knee is bent, such as getting up from a chair or going down the stairs.
Injury Mechanism
The quadriceps tendon is usually injured with a sudden high force across the tendon, such as landing from a jump. The quadriceps tendon can be injured by a direct blow or a sharp laceration across the tendon. Often, the quadriceps tendon is weak prior to the injury due to chronic illness or a period of inactivity.
Symptoms
Quadriceps tendon injuries present as significant pain across the front of the knee, just above the kneecap, and immediate weakness in supporting ones weight while squatting. There is often cramping of the thigh muscles. Patients usually cannot straighten their knee out fully with a complete tear of the quadriceps tendon. Rapid swelling occurs. Often, one can feel a gap above their kneecap at the site of the rupture.
Diagnosis
 The physician’s work-up will start with a careful history and exam. The physician can often feel the defect in the quadriceps tendon and can appreciate the weakness on trying to straighten out the knee against resistance.
The physician’s work-up will start with a careful history and exam. The physician can often feel the defect in the quadriceps tendon and can appreciate the weakness on trying to straighten out the knee against resistance.
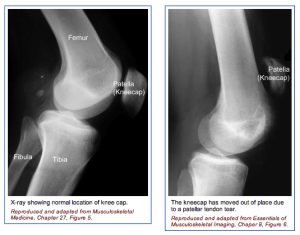
With a complete tear, x-rays reveal a low position of the patella, since the pull of the quadriceps is no longer pulling up on the patella.
An MRI scan is often obtained to confirm the diagnosis, especially if the physician is concerned that the injury may be just a partial tear that may be able to heal without surgical repair. Plain x-rays show the bones of the knee, while MRI scans reveal the soft tissues around the knee including the ligaments, menisci, muscles and tendons.
Treatment
Your physician will discuss treatment options with you. Treatment decisions are based on whether the injury is a complete tear or a partial tear. Partial tears are usually treated with a brace. The brace is initially locked out completely straight to take all of the pressure off of the injured tendon. As healing occurs, the hinges are unlocked and motion and strengthening are initiated. With complete tears, surgery is usually recommended.
Surgery involves sewing the two ends of the tendon together with strong suture material. If the tendon has pulled directly off of the kneecap, drill holes are made into the bone to repair the tendon directly to the bone. Risks and benefits of surgery are discussed thoroughly with the patient.
What to expect after surgery
Quadriceps tendon surgery is usually performed as an outpatient procedure. Patients are sent home with crutches and a knee brace with the knee fully straightened to protect the repair. Depending on the strength of the repair, patients start gentle range of motion and progressive weight bearing over 6-8 weeks.
Patients are using a stationary bike by 2 months, and an elliptical or stair climber shortly thereafter. Jogging is restricted until 4 months following surgery and full sports activities are not resumed until 6 months after surgery. Most patients can return to full activities, with no restrictions and no bracing at the 6th month point.
 Anatomy
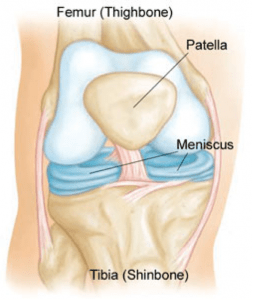
Anatomy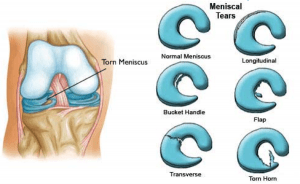 The meniscus is often injured with twisting the knee while in a squatting position. This creates a split or flap to occur while the meniscus is being compressed.
The meniscus is often injured with twisting the knee while in a squatting position. This creates a split or flap to occur while the meniscus is being compressed. 
 Anatomy
Anatomy