
From orthoinfo.aaos.org
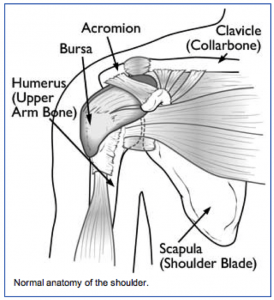
Tendinitis occurs when the tendons of the rotator cuff or the long head of the biceps becomes swollen or inflamed (normally thin fluid filled sack that allows the rotator cuff to glide smoothly under the acromion) becomes swollen or inflamed.
Injury Mechanism: Bursitis and tendinitis are commonly seen in throwing athletes, those doing overhead lifting, or with repetitive motions and overuse of the shoulder. Often, one does not recall a specific injury, but awakens with pain.
Symptoms: When patients have bursitis, they describe pain over the lateral aspect of the shoulder with overhead reaching or laying on that shoulder at night. With tendinitis, pain occurs when using the rotator cuff or biceps in addition to the pain with overhead reaching or laying on that shoulder at night.
Diagnosis: The physician’s work-up will start with a careful history and exam. With tendinitis, the physician can isolate the tendons involved by eliciting pain with use of those tendons plus the impingement test is positive. With bursitis, pain cannot be elicited with use of specific tendons, but the impingement test is still positive.
X-rays are often normal with bursitis or tendinitis, but occasionally a spur is identified on a special “outlet view” that can be obtained in the physician’s office. An MRI scan is sometimes obtained to confirm that the rotator cuff is not torn, especially when patients do not respond to initial treatment.
Treatment: The mainstay of treatment for bursitis and tendinitis is non-surgical. Most patients respond to a short course of anti-inflammatories, stretching, and gentle strengthening of the external rotators of the shoulder. This can be accomplished at home with rubber tubing. If symptoms persist, one can inject the bursa with cortisone to cause the swollen tissues to shrink so they will no longer rub, or impinge.
If the symptoms respond temporarily to the injections, but keep recurring, one can consider surgery to shave down the undersurface of the acromion (acromioplasty) to make more clearance for the rotator cuff and bursa to slide underneath without rubbing. This type of surgery is performed through the arthroscope, using 2 or 3 small incisions, and looking inside the shoulder with a small lens and camera.”
What to expect after surgery: Most shoulder surgery is now performed as an outpatient procedure. In the rare event that an acromioplasty is needed to stop the impingement process, most patients find that they do best by resting their shoulder in a sling for 3 or 4 days following surgery.
They are then encouraged to come out of the sling for gentle stretching exercises. Once comfortable (usually 1 or 2 weeks following surgery), gentle strengthening is initiated with rubber tubing. Once the patient is off of his/her medication, they can resume driving and returning to office work. Most patients can return to full activities in 6 to 8 weeks.