
 Description
Description
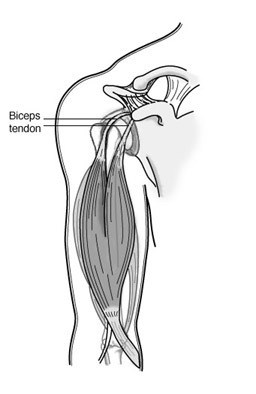
Tennis elbow is a degenerative condition of the tendon fibers that attach on the bony prominence (epicondyle) on the outside (lateral side) of the elbow. The tendons involved are responsible for anchoring the muscles that extend or lift the wrist and hand (see Figure 1).
Risk Factors/Prevention
Tennis elbow happens mostly in patients between the ages of 30 years to 50 years. It can occur in any age group. Tennis elbow can affect as many as half of athletes in racquet sports. However, most patients with tennis elbow are not active in racquet sports. Most of the time, there is not a specific traumatic injury before symptoms start. Many individuals with tennis elbow are involved in work or recreational activities that require repetitive and vigorous use of the forearm muscles (see Table 1). Some patients develop tennis elbow without any specific recognizable activity leading to symptoms.
Symptoms
Patients often complain of severe, burning pain on the outside part of the elbow. In most cases, the pain starts in a mild and slow fashion. It gradually worsens over weeks or months. The pain can be made worse by pressing on the outside part of the elbow or by gripping or lifting objects. Lifting even very light objects (such as a small book or a cup of coffee) can lead to significant discomfort. In more severe cases, pain can occur with simple motion of the elbow joint. Pain can radiate to the forearm.
To diagnose tennis elbow, tell the doctor your complete medical history. He or she will perform a physical examination.
- The doctor may press directly on the bony prominence on the outside part of the elbow to see if it causes pain.
- The doctor may also ask you to lift the wrist or fingers against pressure to see if that causes pain.
 X-rays are not necessary. Rarely, MRI (magnetic resonance imaging) scans may be used to show changes in the tendon at the site of attachment onto the bone.
X-rays are not necessary. Rarely, MRI (magnetic resonance imaging) scans may be used to show changes in the tendon at the site of attachment onto the bone.
Treatment Options
In most cases, nonoperative treatment should be tried before surgery. Pain relief is the main goal in the first phase of treatment. The doctor may tell you to stop any activities that cause symptoms. You may need to apply ice to the outside part of the elbow. You may need to take acetaminophen or an anti-inflammatory medication for pain relief.
Orthotics can help diminish symptoms of tennis elbow. The doctor may want you to use counterforce braces and wrist splints. These can reduce symptoms by resting the muscles and tendons (see Figure 2).
Symptoms should improve significantly within four weeks to six weeks. If not, the next step is a corticosteroid injection around the outside of the elbow. This can be very helpful in reducing pain. Corticosteroids are relatively safe medications. Most of their side effects (i.e., further degeneration of the tendon and wasting of the fatty tissue below the skin) occur after multiple injections. Avoid repeated injections (more than two or three in a specific site).
 After pain is relieved, the next phase of treatment starts. Modifying activities can help make sure that symptoms do not come back. The doctor may want you to do physical therapy. This may include stretching and range of motion exercises and gradual strengthening of the affected muscles and tendons (see Figure 3). Physical therapy can help complete recovery and give you back a painless and normally functioning elbow. Nonoperative treatment is successful in approximately 85 percent to 90 percent of patients with tennis elbow.
After pain is relieved, the next phase of treatment starts. Modifying activities can help make sure that symptoms do not come back. The doctor may want you to do physical therapy. This may include stretching and range of motion exercises and gradual strengthening of the affected muscles and tendons (see Figure 3). Physical therapy can help complete recovery and give you back a painless and normally functioning elbow. Nonoperative treatment is successful in approximately 85 percent to 90 percent of patients with tennis elbow.
Treatment Options: Surgical
Surgery is considered only in patients who have incapacitating pain that does not get better after at least six months of nonoperative treatment.
The surgical procedure involves removing diseased tendon tissue and reattaching normal tendon tissue to bone (see Figure 4). The procedure is an outpatient surgery; you do not need to stay in the hospital overnight. It can be performed under regional or general anesthesia.
Technique for surgical treatment of lateral epicondylitis. A, Skin incision over the lateral epicondyle. B, Distal reflection of the extensor mechanism exposing the lateral compartment of the elbow. C, Excision of pathologic tissue from the underside of the extensor mechanism. D, Decortication of the lateral epicondyle. E, Drilling of two V-shaped tunnels within the lateral epicondyle. F, Reattachment of the extensor mechanism to the lateral epicondyle. G, Side-to-side repair of the extensor tendon mechanism.
Most commonly, the surgery is performed through a small incision over the bony prominence on the outside of the elbow. Recently, an arthroscopic surgery method has been developed.
So far, no significant benefits have been found to using the arthroscopic method over the more traditional open incision.
After surgery, the elbow is placed in a small brace and the patient is sent home. About one week later, the sutures and splint are removed. Then exercises are started to stretch the elbow and restore range of motion. Light, gradual strengthening exercises are started two months after surgery. The doctor will tell you when you can return to athletic activity. This is usually approximately four months to six months after surgery. Tennis elbow surgery is considered successful in approximately 90 percent of patients.
 Risk Factors/Prevention
Risk Factors/Prevention  In appropriately selected patients, the improvement in pain and function can be dramatic. With an experienced surgeon, the results of elbow replacement are the same as the results of hip replacement and knee replacement. For patients who are too young or who are too active to have prosthetic joint replacement, there are other reasonably good options.
In appropriately selected patients, the improvement in pain and function can be dramatic. With an experienced surgeon, the results of elbow replacement are the same as the results of hip replacement and knee replacement. For patients who are too young or who are too active to have prosthetic joint replacement, there are other reasonably good options. 
 Diagnosis and treatment
Diagnosis and treatment