
Most people are familiar with joint replacement surgery for the hip, knee, and shoulder joints. Joint replacement surgery in the wrist is less common but can be an option if you have painful arthritis that does not respond to other treatments.
Anatomy of the wrist
The wrist is a more complicated joint than the hip or the knee. At the base of the hand are two rows of bones, with four bones in each row. These are called the carpals. The long thin bones of the hand radiate out from one row of carpals toward the fingers and thumb. The two bones of the lower arm (radius and ulna) form a joint with the other row of carpals. All the bone ends are covered with a slick, elastic tissue called cartilage, which enables the bones to move smoothly against each other. However, if the cartilage is worn away or damaged by injury, infection or disease, the bones will rub against each other causing pain. During any total joint replacement, the worn-out bone ends are removed and replaced by an artificial joint (prosthesis).
Reasons for wrist replacement surgery
The typical candidate for wrist replacement surgery has severe arthritis but does not need to use the wrist to meet heavy demands in daily use. The primary reasons for wrist replacement surgery are to relieve pain and to maintain function in the wrist and hand.
- Osteoarthritis, the most common form of arthritis, results from a gradual wearing away of the cartilage covering on bones.
- Rheumatoid arthritis is a chronic inflammatory disease of the joints that results in pain, stiffness and swelling. Rheumatoid arthritis usually affects several joints on both the right and left sides of the body.
Both forms of arthritis may affect the strength of your fingers and hand, making it difficult for you to grip or pinch. In some cases, fusing the wrist bones together will reduce or eliminate pain and improve grip strength. However, if the bones are fused together, you will not be able to bend the wrist. Wrist replacement surgery may enable you to retain or recover wrist movements and improve your ability to perform daily living activities, especially if you also have arthritis in the elbow and shoulder.
Implant design
Wrist implants are made of the same kind of materials used for hip and knee joint replacements. There are several different designs. Most have two components and are made of metal; a high quality plastic called polyethylene is used as a spacer between the two components. Newer implant designs try to replicate the anatomy of the wrist.
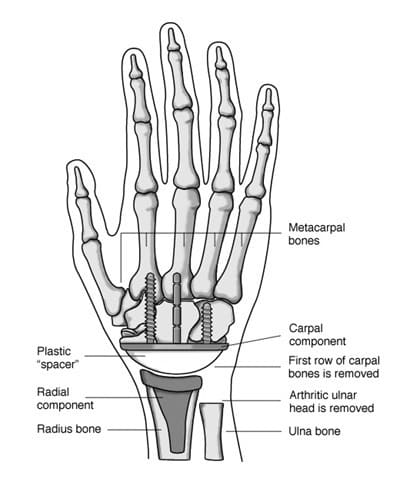
The piece that attaches to the lower arm (radius bone component) fits into the bone of the lower arm. The top of this component has a curve that matches to the wrist part. The piece that attaches to the hand (carpal component) may have one long stem and one or two shorter stems that insert into the hand bones, or use small screws. The surface of this component is flat. The plastic spacer comes in different sizes so it can be matched to your hand. It is normally flat on one side and rounded on the other. This design enables it to fit into the carpal component while it rocks on the radial component, creating a more natural wrist motion.
Implant insertion
A wrist joint replacement can be done as an outpatient procedure, unlike a hip or knee replacement. Wrist replacement surgery is often combined with other procedures to correct deformities or disorders in the tendons, nerves, and small joints of the fingers and thumb.
The incision is made on the back of the wrist. The damaged ends of the lower arm bones are removed and the first row of carpal bones may also be removed. The radial component of the prosthesis is inserted into the center of the radius bone on the outside of the lower arm. It is held in place with bone cement. Depending on the component design, the carpal component is then inserted into the center hand bone (third metacarpal) or screwed into the remaining row of carpal bones. Bone cement may be used to hold the component in place. The carpal bones may be linked or fused together to better secure this component.
An appropriately sized spacer is used between the metal components.
After your surgery
You will have to wear a cast for the first several weeks. When the cast is removed, you will have to wear a protective splint for the next six to eight weeks. Although pain relief is immediate, you will have to do gradual exercises for several weeks to restore movement and, eventually, to increase power and endurance. Wrist arthroplasty can improve motion to about 50 percent of normal.
The physical demands that you place on the wrist prosthesis will have an effect on how long the implant lasts. You will not be able to use a hammer often or pneumatic tools. You may only be able to lift a limited amount of weight. A fall on the outstretched hand may break the prosthesis, just as it might fracture a normal wrist. So you will want to avoid activities such as roller sports that could result in a fall.
Although there have been significant advances in wrist prostheses, the implant may loosen or fail due to wear or deformation. In these cases, additional surgery may be necessary. On average, a wrist replacement can be expected to last 10 to 15 years with careful use. As with all implants, long-term follow-up is advised. Generally, you should see your hand surgeon every year or two years so that x-rays can be taken and used to identify any developing conditions or problems.
 Description
Description  Sometimes, a broken scaphoid does not show up on an X-ray right away. When this is the case, the doctor may put your wrist in a splint and wait to take a new X-ray in a week or two, when the fracture may become visible. Keep the splint on and do not do any heavy lifting during the waiting time.
Sometimes, a broken scaphoid does not show up on an X-ray right away. When this is the case, the doctor may put your wrist in a splint and wait to take a new X-ray in a week or two, when the fracture may become visible. Keep the splint on and do not do any heavy lifting during the waiting time.

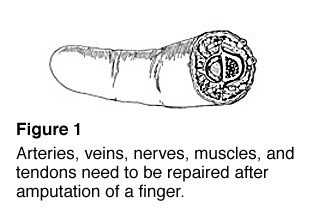 Replantation is usually recommended when the replanted part will work at least as well as a prosthesis. Generally, a missing hand would not be replanted knowing that it would not work, be painful, or get in the way of everyday life. Before surgery the doctor, if possible, will explain the procedure and how much use is likely to return following replantation. The patient or family member must decide whether that amount of use justifies the long and difficult operation, time in the hospital, and months or years of rehabilitation.
Replantation is usually recommended when the replanted part will work at least as well as a prosthesis. Generally, a missing hand would not be replanted knowing that it would not work, be painful, or get in the way of everyday life. Before surgery the doctor, if possible, will explain the procedure and how much use is likely to return following replantation. The patient or family member must decide whether that amount of use justifies the long and difficult operation, time in the hospital, and months or years of rehabilitation.