Softball pitching subjects the biceps to high forces and torques when the player’s arm swings around to release the ball. Published in the March 2009 issue of the American Journal of Sports Medicine, the study of the “windmill” pitching motion appears to explain the high incidence of anterior shoulder pain observed in female softball players.
In the study, seven women — three collegiate and four professional pitchers — underwent motion analysis and surface electromyography to evaluate the muscle firing pattern of their biceps in the course of a windmill pitch. Electromyography detects electrical potential generated by muscle cells when they contract.
The researchers found that even though the upper arm movement in both baseball and fast-pitch softball gives the ball about the same velocity, the muscle force during the windmill pitch was much higher, according to the press release.
Moreover, the maximum force, or maximum contraction, occurred not when the arm was cocked, as in baseball’s overhand pitching, but when the arm circled around from the 9 o’clock position (i.e. almost fully extended back) to the 6 o’clock position (i.e. perpendicular with the ground), completing the windmill motion with the release the ball.
In one case, a pitcher had ruptured her tendon during play, which implicated the long head of the biceps tendon as the source of stress. Female softball pitchers are prone to overuse injury not only because of windmill pitching dynamics, but also because they pitch so many games.
Common Softball Injuries
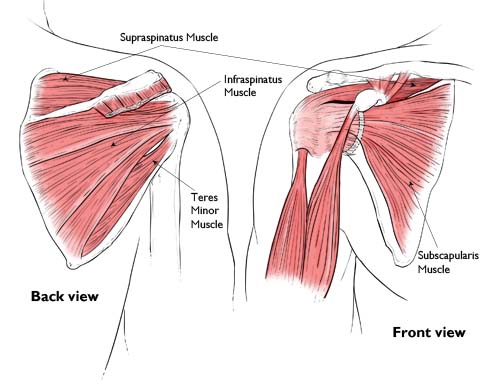
Common injuries in softball players include tendonitis, rotator cuff and tendon strain, and ulnar nerve damage, but there are also plaguing lower body injuries that affect softball pitchers. So what is the source of injury? In simplest terms, the hips provide the platform for the scapula, and the scapula is the platform for the shoulder. If there is dysfunction in that system, this leads to injury. If a pitcher complains of shoulder pain, the shoulder may not be at fault for the pain, but rather faulty mechanics in the lower body.
Many times, softball pitchers experience upper body injuries that may be a result of faulty lower body mechanics. Force is produced in the ground, transfers through the legs and torso, and finishes in the upper body. If something along those lines isn’t functioning properly, injury will present itself.
Anterior shoulder pain is one of the most common complaints among windmill pitchers. A typical overhand pitch sees around 108 degrees of motion, whereas the windmill pitch has around 360 degrees of motion; which is an increase in the eccentric action of the biceps.
Strength and conditioning for softball pitchers takes on a significant meaning because all of the energy is transferred from the ground up to the hand (the final point of contact with the ball) and pitch from a flat surface vs. baseball players who pitch off of a mound; this means that a softball pitcher would need to train in ground reaction-force, emphasizing gluteal exercises. Strong glutes will provide a strong base for the pelvis, then transferring energy through the core to the upper body.
When considering training regimens for windmill softball pitchers, much of the conditioning should focus on strengthening the lower extremity and lumbopelvic-hip complex. The lower extremities and lumbopelvic-hip musculature can often be addressed in the same exercises. Ideally, the lumbopelvic-hip complex should be addressed first in the training cycle in order to maintain a base of stability throughout all the conditioning exercises.
Dr. Shapiro states, “Warming up prior to the game and using the proper technique while playing will reduce the opportunity for injury; however, if you are experiencing pain this may be from overuse or an acute injury. It is best to seek medical attention and be evaluated by an Orthopedic and Sports Medicine Specialist.”
If you believe you are suffering from a softball-related injury and need specialized orthopedic care, Orthopedic Specialists of Seattle provide excellent treatment options available for you.